Artefacts and patient stories: a qualitative exploration of the diabetic foot ulcer journey in Singapore
Received:
Accepted:
Published:
Authors: Keith Rui Yi Lee, Yu Da Wong, Dexter Yak Seng Chan, Chelsea Chiew Chie Law, Hannah Woon Ching Leong, Jo Ann Huey Ping Lim, Jaime Hui Xian Lin, Yuan Teng Cho, Shaun Wen Yang Chan, Chee Wei Lee, Sadhana Chandrasekar, Zhiwen Joseph Lo
Citation:
Lee K et al, (2026) Artefacts and patient stories: a qualitative exploration of the diabetic foot ulcer journey in Singapore. Global Wound Care Journal 2 (1): 32-39.
The authors have no conflict of interest to declare.
Funding:
Woodlands Health Small Projects Utilising Teams (SPROUTS) grant number: SPR3-22-CII-01.
Acknowledgements:
The authors thank Robert Sia, Nancy Siaw and Ang Kim Keow for their support.
Authors’ contributions:
DYSC, CCCL, HWC, JAHPL, JHXL, YTC, SWYC, CWL, SC and ZJL carried out patient recruitment and data collection; KRYL and YDW carried out data analysis and wrote the article. All authors contributed to review and editing of the final manuscript.
Corresponding author:
Keith Rui Yi Lee, Wound and Vascular Centre, Woodlands Health, Singapore, 17 Woodlands Drive , Singapore, 737628. Email: ruiyikeith@gmail.com
DOI
10.63896/gwcj.2.1.32
Background: The lived experiences of people with diabetic foot ulcers (DFUs) are rarely studied through artefact based approaches. Patient artefacts can help reify experiences and memories and elicit information that is not easily accessed by other methods, providing new insights into psychosocial impacts, coping strategies, and patient advice to peers.
Aim: To analyse the lived experiences of DFU patients, through artefacts and accompanying narratives.
Methods: At an outpatient multidisciplinary podiatry clinic, 10 DFU patients each contributed a personal artefact symbolising their DFU journey, and completed an accompanying open-ended survey. Artefacts and data were analysed via reflexive thematic analysis, with the social-ecological model (SEM) as an organising and sensitising framework.
Results: Artefacts helped paint a richer picture of the experiences of DFU patients, elicit emergent findings from narratives, and symbolise key aspects of lived experiences. Participants reported a wide range of impacts, both to their lives and those of their caregivers, and were willing to share advice, based on their DFU journeys, with other patients.
Conclusion: Artefacts and their accompanying stories provide a richer picture of, and insights into, DFU patient experiences, meriting further exploration in qualitative studies of people with DFUs.
Diabetic foot ulcers (DFUs) are among the most devastating complications of diabetes, affecting up to 25% of people with the condition during their lifetime (Amin and Doupis, 2016). DFUs not only carry significant morbidity, risk of amputation and poor clinical outcomes (Wukich and Raspovic, 2018), but also impose significant psychological, social and economic burdens on patients and their families due to the likelihood of amputation, heightened frequency of outpatient and emergency department visits, and the demands of home care (Lo et al, 2021; Riandini et al, 2022; Zhang et al, 2016).
The psychological and social aspects of DFUs, including the quality of life and lived experiences of patients, are often studied through the use of patient-reported experience measures (PREMs) and patient-reported outcome measures (PROMs) (Garratt et al, 2005; Hu et al, 2017; Shunmuga Sundaram et al, 2022; Gilmore et al, 2023), as well as qualitative studies which provide more open-ended explorations of patient experiences.
One underutilised method of exploring the lived experiences of individual patients is through the use of patient artefacts. Artefacts not only help to reify and share experiences and memories, but are also imbued with meaning as they are woven into our everyday lives, a process underscored by Turkle’s (2007) concept of ‘evocative objects’. This suggests that incorporating artefacts into qualitative studies may help to elicit information not readily accessed by other methods (Heersmink, 2018), as illustrated by empirical studies showing that artefact-based interviews facilitate reflection, co-creation of experiences, and visualisation between interviewer and interviewee (Tuan, 1980; Csikszentmihalyi, 1993; Akama et al, 2007).
Artefacts thus represent a rich, but hitherto untapped, resource for exploration of the lived experiences of people with DFUs; an artefact-based approach to qualitative study has the potential to yield new insights that could enhance patient education, inform health services design, and provide peer-to-peer support within wound care communities.
While several studies have previously used photo-elicitation and photovoice methods to explore the experiences of people with diabetes, particularly adolescents with type 1 diabetes (Fritz and Lysack, 2014; Florian et al, 2015; Peña-Purcell et al, 2017; Malik et al, 2021; Nettleton et al, 2022; Tang et al, 2025), to our knowledge, no existing studies involving DFU patients have used our artefact-based approach.
Aim
This study aimed to fill the existing gap in the literature by documenting and analysing anonymised patient artefacts and accompanying narratives. By exploring the lived experiences, the study sought to better understand the psychosocial impacts, coping strategies, and patient advice to peers related to their DFU journey.
Ethics committee approval
Ethics approval was obtained from the National Healthcare Group Domain Specific Review Board (2022/00743), and all patients provided written informed consent for participation and for artefact use.
Methods
This qualitative substudy formed part of a broader investigation on patient experiences with DFUs at a tertiary care institution in Singapore which provides multi-disciplinary clinics for people with DFUs (Lam et al, 2025).
Study design
This study used a descriptive qualitative research design with an orientation towards phenomenology. Because of the limitations of the data collection methods utilised in the larger study, it was determined that the methodology could not formally be considered as phenomenological analysis; however, the aims, epistemological underpinnings, and analytical methods of this study were consistent with a phenomenological approach (Laverty, 2003; Ajjawi and Higgs, 2007; Smith and Osborn, 2008). The research questions for this study were addressed within a paradigmatic framework of constructivism. An experiential orientation to data was adopted. The analysis used both inductive and deductive approaches, with semantic coding of data.
Sampling and recruitment
Fifty patients with DFUs, who were reviewed at an outpatient multidisciplinary podiatry clinic within a tertiary hospital in Singapore from January 2023 to April 2023, were invited to complete an anonymised survey and, if willing, to contribute a personal artefact symbolising their DFU journey. Inclusion criteria were: a diagnosis of diabetes with a foot ulcer at or distal to the malleolus; age between 21 and 90 years; the ability to provide written informed consent; proficiency in English or access to family members to act as interpreters; and the submission of an artefact as part of the survey. Exclusion criteria were: the absence of a clinical diagnosis of diabetes or a foot ulcer; an inability to provide consent; refusal to participate in the study; lack of English proficiency without access to a family members to act as interpreter; presence of cognitive impairment; and opting out of the artefact-based component.
Data collection
The survey consisted of five open-ended questions [Appendix A] (access via QR code in the PDF of this article) for patients, which explored:
- their personal journey with diabetes and DFU;
- the recognition and onset of DFU;
- the impact on family and lifestyle;
- a symbolic artefact representing their DFU experience; and
- their advice to peers.
All stories and artefacts were anonymised and infection-control measures were adhered to where appropriate. Responses and artefacts were not returned to participants for further comments and/or analysis.
Data analysis
Artefacts and data from the survey transcripts were analysed using Braun and Clarke’s (2006) reflexive thematic analysis; this process was informed by phenomenological analysis and applied flexibly and iteratively. Bronfenbrenner’s (1979) social-ecological model (SEM) provided a framework for identification of themes and further analysis.
The SEM framework relates individual behaviours to different levels of systems, e.g. micro, meso and macro, and has previously been used in both DFU (Zhu et al, 2023) and broader diabetes (Whittemore et al, 2004; Hill et al, 2013) research. Following data familiarisation and an initial inductive round of coding, the SEM was used as an organising framework for re-analysing, reorganising and renaming the consolidated themes, as well as acting as a framework to sensitise the coder to other theoretical concepts which may have been missed during the first round of coding. This helped to avoid limiting the themes that could be identified from the data, while also allowing sensitisation to specific concepts highlighted in the SEM.
The data were then revisited and recoded using the updated codes; the final consolidated codes formed the basis of the study’s data analysis.
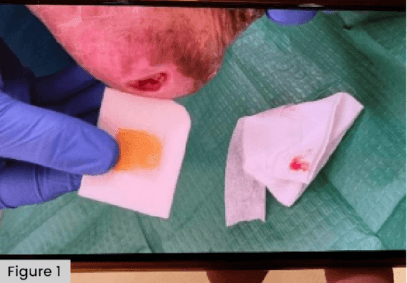
Figure 1. An artefact in the form of a wound photograph and wound dressing equipment, submitted by P003.
Results
Participants
Of the 50 patients involved in the larger study, 10 submitted artefacts and narratives for analysis. Some participants submitted more than one artefact. In total, 10 anonymised participant stories and 12 distinct artefacts were analysed. Participants were identified based on their IDs from the larger study.
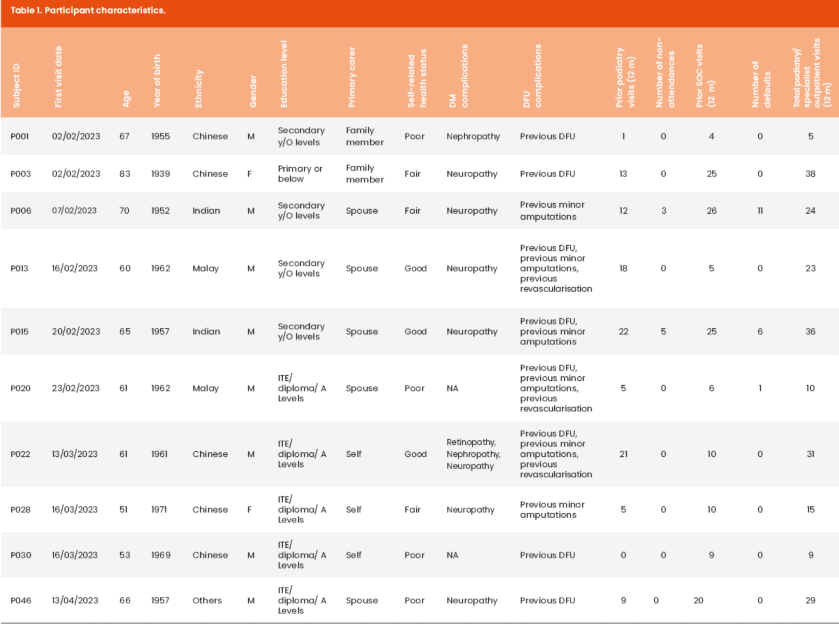
Participant characteristics are displayed in Table 1. Of the 10 participants, 80% were men. Patients had a median age of 63 years (mean 63.7, IQR 60–67, range 51–83). Seven (70%) had a spouse or other family member as their primary carer. Three described themselves as their own primary carer. Four reported their health status as ‘poor’, three as ‘fair’, and three as ‘good’. The median total number of visits to podiatry and/or specialist outpatient clinic services in the past 12 months (minus non-attendances) was 23.5 (mean 22, IQR 10–31, range 5–38).
Artefacts
Artefacts submitted for analysis included:
- Wound photographs (n=6).
- Wound dressing packaging (n=3).
- DFU footwear (n=1).
- Glucose sachets (n=1).
- Urine container (n=1).
Thematic findings
Symbolism of artefacts
Patients were asked to submit an artefact that ‘best describes your journey with diabetic foot ulcers’. These artefacts were analysed as indicative of patients’ primary preoccupations regarding living with DFUs, and were categorised according to the following three themes, which were informed, but not restricted, by the SEM framework:
1. Individual: impact to self
In particular, the submission of wound photographs suggested that the patients’ primary preoccupation with DFUs was at an individual level. This suggested either continued pain, personal inconvenience (e.g. due to lack of mobility) or impact on self-image.
2. Individual: quality of life
DFU footwear was seen as a step down in quality of life, impinging on the patient’s daily activities and mobility, as the patient who submitted this artefact reported that he had lost his job after undergoing toe amputation.
3. Microsystem: daily burdens to self and others
Wound dressing packaging, glucose sachets and urine containers represented tools that people with DFUs had to use or be aware of every day. They symbolised the need for constant vigilance and attention to DFUs of both patients and their primary caregivers.
Analysing artefacts in relation to patient narratives
Themes within the artefacts commonly recurred in and complemented the accompanying participant narratives, adding a further dimension and richness to these accounts. Two specific examples are given to illustrate this.
The first example is P001, who submitted his wound dressing packaging [Figure 1]. The biggest impact of this patient’s DFU was the increased caretaking burden on his family members, who had to care for him at home and accompany him on regular clinic visits. This aligns with the wound dressing packaging being symbolic of the everyday tasks and burdens associated with DFUs, and paints a more complete picture of the participant’s primary perception that his DFU imposed changes to his caregivers’ daily schedule. This allowed analysis of emergent findings, such as suggestions of guilt and/or responsibility felt by the participant towards his caregivers because of this burden.
The second example is P015, who donated his DFU footwear [Figure 2]. In his narrative, this patient explained that he was unable to continue working due to the condition of his foot, which increased his family’s financial burden in addition to caretaking duties. The DFU footwear thus came to symbolise not only loss of mobility and quality of life, but also the subsequent effects that the DFU had on him and his microsystem, and the social determinants of health regarding this condition. This participant’s advice to other people with DFUs was not to downplay or be oblivious to their own condition, or to imagine that their wounds are not serious. The artefact and accompanying narrative were symbolic of the participant’s loss of mobility and the consequences of that loss, thus adding weight to his advice.

Figure 2. An artefact of DFU footwear submitted by P015.
These two examples illustrate how the artefacts not only provided a richer and fuller picture of patients’ lived experiences, complementing patient narratives and generating themes for further exploration, but were also representational of DFU journeys, symbolising participants’ preoccupations, narratives, and advice for other patients.
The range of impacts of DFUs
One finding that emerged from participants’ narratives was that DFUs could impact individuals in a varied and wide ranging way. These impacts fell within the individual and microsystem levels, categorised as follows:
- No impact: Two participants reported that there was ‘no impact’ on their life, because they were still able to work and live independently.
- Impact on individuals: Participants reported fewer impacts on themselves; the most common impact was the inconvenience of attending regular clinic appointments, due to the disruption to their own schedule and the travel time required. One patient had to stop working.
- Impact on microsystems: The most frequent impact described was on primary caregivers and family (spouses, children, or helpers), due to participants’ reliance on them for wound dressing and accompaniment to clinic visits. Repeated dressing changes, transport, and clinic visits caused logistical difficulties, work-related inconvenience, and imposed emotional stress for caregivers, who often had to take time out from their own schedules and time off work in order to provide care. Several patients reported that their family members suffered additional financial burdens due to the cost of regular treatment and visits, despite some relief through national savings schemes.
Advice to others
Several themes were consistently identified in participants’ advice to other people with DFUs. The most common advice given related to maintaining diabetes control and lifestyle modification. six participants advised long-term lifestyle changes such as monitoring one’s diet, adhering to medication schedules, and exercising; one also mentioned quitting smoking and drinking alcohol. Other advice included listening to doctors, seeking early medical attention for wounds, having a positive attitude about their condition, and sharing their suggestions on wound management. All advice was targeted at the level of the individual.
In several cases, patients’ advice to others was noted to relate strongly to their own (negative) experiences. For example, P006 suffered from poor diabetes control over the course of his diabetes journey due to lack of concordance to medication and advice from healthcare professionals; his DFU wound condition only started improving after he began taking medications and heeding advice. His advice to other patients was to control their diabetes and adhere strictly to their medication schedule. This suggests the potential for communities in which people with diabetes can share their stories and advice. A valuable patient education resource such as this could help patients to learn from each other’s journeys to avoid potential pitfalls.
Emotional responses
Participants’ narratives highlighted their frustration and guilt, but also their positivity and resilience towards family and healthcare providers. Common causes of frustration and guilt involved the increased caretaking and financial burden imposed on participants’ primary caregivers. Other participants expressed continued positivity and resilience towards their wounds, for example by advising other patients not to worry excessively about their condition (P028) and to ‘think positively’ (P030).
Discussion
This study qualitatively explored the lived experiences of 10 DFU participants by analysing artefacts representative of their DFU journey, along with accompanying narratives and advice to other DFU patients. Artefacts helped to paint a richer picture of participants’ journeys with DFUs, elicit emergent findings from narratives, and symbolise key aspects of lived experiences. Participants with DFUs reported a wide range of impacts on their lives, and varied emotional responses, highlighting the diversity of patient experiences.
The advice from participants to other patients revolved around maintaining diabetes control and lifestyle modification and listening to their doctors, and in some cases related strongly to participants’ own experiences.
The novel artefact-based approach used in this study is, to the best of the authors’ knowledge, the first time that lived experiences of people with DFUs have been investigated using multimodal interview methods. The most similar methods to this, namely photo-elicitation and photovoice, have been previously used in research on diabetes and other chronic illnesses (Lal et al, 2012; Teti et al, 2012); and were found to elicit rich, context-specific, and highly reflective data not readily accessed by other methods, and also to empower interviewees to actively tell their stories (Harper, 2002; Lorenz, 2011; Fritz and Lysack, 2014; Peña-Purcell et al, 2017).
In this study, the artefact-based approach similarly yielded richer and fuller pictures of participants’ experiences, as they reified participants’ lived experiences when contextualised with accompanying narratives. By making abstract memory and emotion concrete, artefacts became symbols for participants’ unique lived experiences with DFUs, in line with Turkle’s (2007) ‘evocative objects’. Patient-submitted artefacts also amplified the voice of patients in a way that complements structured PREMs. Where PREMs tend to use multiple-choice questionnaires, allowing patients to select and submit artefacts themselves can empower patients to participate in defining which aspects of their lived experiences are important to them.
The findings align with prior literature showing that DFUs impose significant psychosocial and financial burdens. Previous research exploring the lived experiences of people with DFUs, and the impact of DFUs beyond clinical outcomes, found that patients often report increased dependence on others, financial burden, and guilt due to the increased caretaking burden on primary caregivers (Coffey et al, 2019; Oni, 2020; Crocker et al, 2021; Ma et al, 2023); these themes were prominent in the reported impacts of some participants in this study.
One finding from this study, which is under-emphasised in the literature, is that the way DFU impacts on different patients’ lives is wide ranging – from no reported impact to disruption of life, job and family. Few studies address the range of disruption experienced (Kuang et al, 2021); qualitative studies of lived experiences tend to focus on how, rather than whether, DFUs have impacted patients’ lives. Future research could investigate factors associated with the greater or smaller impacts of DFUs (and lower extremity amputations) on patients’ lives.
The study found that participants sometimes based their advice to other patients on learning points from their own journeys, which mirrors findings regarding support groups for diabetes that show peer support can facilitate the sharing of experiential knowledge (Mead and MacNeil, 2006) and can potentially have positive impacts on certain clinical and non-clinical outcomes, such as symptoms of hypo- and hyperglycaemia, physical activity/fitness, and healthier eating habits (Dale et al, 2012). Limited literature on support groups for people with DFUs suggest that they may have a positive impact on patients’ knowledge, attitudes and foot care practices (Sharma and Khan, 2021). There may be value in establishing communities of people with DFUs, where members can learn from one another on topics such as self-care, avoiding poor outcomes, and/or improving early recognition of deterioration.
The limitations of this study include its small sample size and single-centre recruitment; the sample represents a relatively narrow demographic of people with DFUs, and may not be representative of other contexts. A reliance on English meant that participants who lacked proficiency in English had to use interpreters. This may have, for some patients, resulted in a loss of nuance or fidelity depending on the interpreter’s skills. Furthermore, as this substudy was part of a larger investigation, opportunities for in-depth qualitative interviews were limited, which restricted opportunities for phenomenological analysis. Future artefact-based studies may benefit from phenomenological interview and analytical methods, as well as methodologies similar to those used in photo-elicitation studies (Plunkett et al, 2013; Fritz and Lysack, 2014; Nettleton et al, 2022) in which participants are invited back for interviews to discuss the artefact. Nonetheless, the findings from this study highlight the value of artefact-based approaches in wound care research and clinical education, and suggest value in further exploration of this methodology in DFU and diabetes research.
Conclusion
The journeys of people with DFUs are often studied through their words, but artefacts can encapsulate and embody challenges and adaptations, elicit information not readily yielded through other methods, and empower patients to define their own experiences beyond PREMs and PROMs questionnaires. Patient artefacts and their accompanying stories can provide a window into the preoccupations, frustrations, adaptations and resilience patients demonstrate in their DFU care journey, meriting further exploration as a method of enhancing patient engagement, peer education and service design in Asia. Our findings also suggest value in future research investigating factors associated with the greater or lesser impacts of DFUs on patients’ lives; the effectiveness of peer communities for support and learning in improving clinical outcomes or PROMs; and the effectiveness of artefact-based storytelling as an educational resource within those peer group settings.
