Delafloxacin in diabetic foot infections involving bone: A mini-review and case series of real-world use
Received:
Accepted:
Published:
Authors: Giovanni Del Fabro, Mariateresa Casarotto, Chiara Zanusso, Astrid Callegari, Federico Giovagnorio, Agnese Zanus-Fortes, Giorgia Abbiati, Rudi Stramanà, Irene Morelli, Giancarlo Basaglia, Barbara Basso, Sergio Venturini
Citation:
Del Fabro G et al, (2026) Delafloxacin in diabetic foot infections involving bone: A mini-review and case series of real-world use. Global Wound Care Journal 2 (1): 48-55.
DOI:
10.63896/gwcj.2.1.48
Aim: Delafloxacin, a novel fluoroquinolone with broad-spectrum activity, represents an interesting off label option for diabetic foot infections (DFIs) with bone involvement. We aimed to share our real-world experience with delafloxacin in deep DFIs managed with combined surgical and antibiotic therapy.
Methods: We conducted a single-centre, retrospective observational study with prospective follow-up, including all adult patients treated with delafloxacin for microbiologically confirmed DFI.
Results: Seven patients met the inclusion criteria (two moderate and five severe DFIs). Polymicrobial infections (85.7%) with anaerobic component (71.4%) predominated. All underwent surgical debridement, empirical intravenous therapy, and oral switch to delafloxacin. Median duration of delafloxacin treatment was 21 days (IQR 18–22). No adverse drug events or clinical failures were observed. A literature review identified only one previous case report describing delafloxacin use in DFI with unspecified duration.
Conclusion: Our preliminary experience supports delafloxacin as a safe and effective oral step-down option for the treatment of moderate to severe DFIs with bone involvement.
Delafloxacin is a novel fluoroquinolone (FQ) active against methicillin-resistant Staphylococcus aureus (MRSA), P. aeruginosa and several anaerobic species (Gómez-Zorrilla et al, 2022). In Europe, delafloxacin received approval in October 2019 for the treatment of skin and soft tissue infections and community-acquired pneumonia. Its broad antimicrobial spectrum, favourable bone penetration and demonstrated anti biofilm activity position delafloxacin as a promising therapeutic option for diabetic foot infections (DFIs), particularly those with associated bone involvement (Geremia et al, 2024).
Aim
We aimed to share our real-world experience with delafloxacin in deep DFIs, assessing its tolerability and efficacy.
Methods
Study design, data collection and analysis
A retrospective observational study with prospective follow-up was conducted in our Institution (“Santa Maria degli Angeli” Hospital of Pordenone, Italy), following the STROBE reporting guidelines (von Elm et al, 2007).
We identified all patients (n=7) with DFI receiving delafloxacin from 1 January 2025 to 1 September 2025. Patients were enrolled at the initiation of delafloxacin therapy prescribed by infectious diseases (ID) consultants. Data were double-checked with pharmacy dispensing reports. We included only adult patients (age ≥18 years) with a microbiologically confirmed diagnosis of DFI, defined and classified according to the IGWDF/IDSA 2023 guidelines (Senneville et al, 2024). Minimum follow-up for final inclusion was 60 days after discharge. Exclusion criteria were: lack of informed consent from the patient or legal representative, absence of clinical information from patient or electronic record, no microbiological diagnosis, a concurrent alternative focus of infection, and insufficient follow-up (or lost at follow-up). Concurrent blood stream infection (BSI), if attributable to DFI, and ongoing antibiotic treatment were not exclusion criteria.
Laboratory data for this study were obtained from the electronic health records of our hospital. The follow-up was conducted by regular assessment of the local status, inflammation markers (white blood cell count, WBC and C-reactive protein, CRP) and monthly follow-up appointments, conducted either in outpatient clinics or via telephone, for up to 6 months after discharge. The presence of local signs of infection, fever (with no other reasons), increasing CRP (with no other reasons) or need for surgical revision were considered as treatment failure.
All patients provided informed consent for off-label drug use before participation. The study was conducted in accordance with the Declaration of Helsinki, and informed consent for using personal clinical data for the study purpose was collected from all participants. Ethical approval was waived due to the retrospective nature of data collection. Anonymised data were collected and analysed in a Microsoft Excel database. Categorical variables were reported as frequencies and percentages; continuous variables as median and interquartile range (IQR 1–3).
A review of the English and Italian-language literature on delafloxacin use in DFI was conducted in PubMed/NCBI and Google Scholar. Key search terms were “delafloxacin” cross-referenced with “diabetic foot” OR “bone infection” OR “osteomyelitis”. A total of 49 articles were retrieved. Articles were screened for the following inclusion criteria: adult patients with DFI with bone involvement, a definite microbiological diagnosis, and delafloxacin treatment. All papers that did not specifically comprise cases of DFI (as indicated in the title or abstract) were excluded. After applying these criteria, one paper was finally retrieved from the literature review (Serrudo et al, 2024).
Multidisciplinary treatment protocol
In our institution, DFI patients requiring surgical treatment are routinely managed by vascular surgeons and infectious diseases consultants, following a standard treatment protocol. This was applied to all patients included in the study. All patients underwent revascularisation when indicated, surgical debridement, and microbiological sampling. Broad-spectrum antibiotics were initiated at admission – before surgical intervention and microbiological sampling – only in haemodynamically unstable patients. Infectious disease consultations were systematically performed at three key stages: at the initiation of empiric intravenous therapy, after receipt of microbiological results to guide de-escalation, and before discharge to define oral step-down and treatment duration. Duration of antibiotic treatment was a multidisciplinary team decision based on clinical progress and laboratory findings.
Microbiological sampling and work-up
After surgical debridement and cleansing, pus from deep abscesses and/or bone fragments were collected from each patient for the microbiological evaluation.
Each biopsy was placed in 5 ml of Tryptone Soy Broth (VACUTEST KIMA, Italy), whereas pus samples were collected in eSwab 480CE (Copan Italia, Italy); a volume of 60 ul of the suspension was inoculated on blood agar, MacConkey agar, Columbia CNA agar and Sabouraud agar (VACUTEST KIMA), respectively; plates were then incubated at 37ºC overnight. For the isolation of fastidious and anaerobic bacteria chocolate agar and Schaedler agar (VACUTEST KIMA) were inoculated with 60 ul of the sample suspension and incubated at 37°C for 48 hours in CO2 and anaerobic atmosphere, respectively.
Simultaneously, blood samples were collected from those patients suspected of having bacteraemia (fever above 38ºC) in BACT/ALERT FA Plus (Aer) and BACT/ALERT FA Plus (Ana) bottles for the isolation of aerobic and anaerobic bacteria, respectively. Incubation was carried out in BACT/ALERT VIRTUO System (bioMérieux, Italy) for maximum 5 days. One uL of positive samples was inoculated in the above reported agar plates that were incubated at the same conditions.
The identification of grown bacteria was performed by Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry (MALDI TOF-MS) (VITEK-MS, BioMérieux, France).
For isolates from pus and bone samples the antimicrobial susceptibility testing (AST) was set up using VITEK2 System (bioMérieux, Italy), following the manufacturer’s instructions. In cases of resistance to FQs and availability of the EUCAST clinical breakpoints for that isolate, delafloxacin susceptibility testing (Delafloxacin E-test, BioMérieux, France) was performed (available in the laboratory from August 2025).
For bacteria isolated from blood culture, AST was carried out in broth microdilution using MicroScan WalkAway 40 plus (Beckman Coulter, US), following the manufacturer’s instructions.
Susceptibility to antimicrobial agents was evaluated for all isolates according to the EUCAST clinical breakpoints v. 14.0.
Results
Seven patients receiving delafloxacin as oral treatment for DFI were included in the study [Figure 1]. Median age was 67 years (IQR 66–79.5), and 71.4% were men. Median Charlson comorbidity index was 5 (IQR 5-7). All patients had a diagnosis of DFI with bone involvement (two classified as moderate, five as severe). Two patients presented with haemodynamic instability (associated with concurrent bloodstream infection in both cases) and started antibiotics before surgical source control. The infection was polymicrobial in six patients (85.7%) and anaerobic bacteria were isolated in the majority of cases (5/7, 71.4% of patients) [Table 1]. As shown in Figure 2, anaerobes constituted the majority of the isolates globally (35%), followed by Enterobacteriaceae, Streptococci and Staphylococci (25%, 20% and 15% of all isolates, respectively). More details are provided in Supplementary Material (Scan the QR code in PDF).
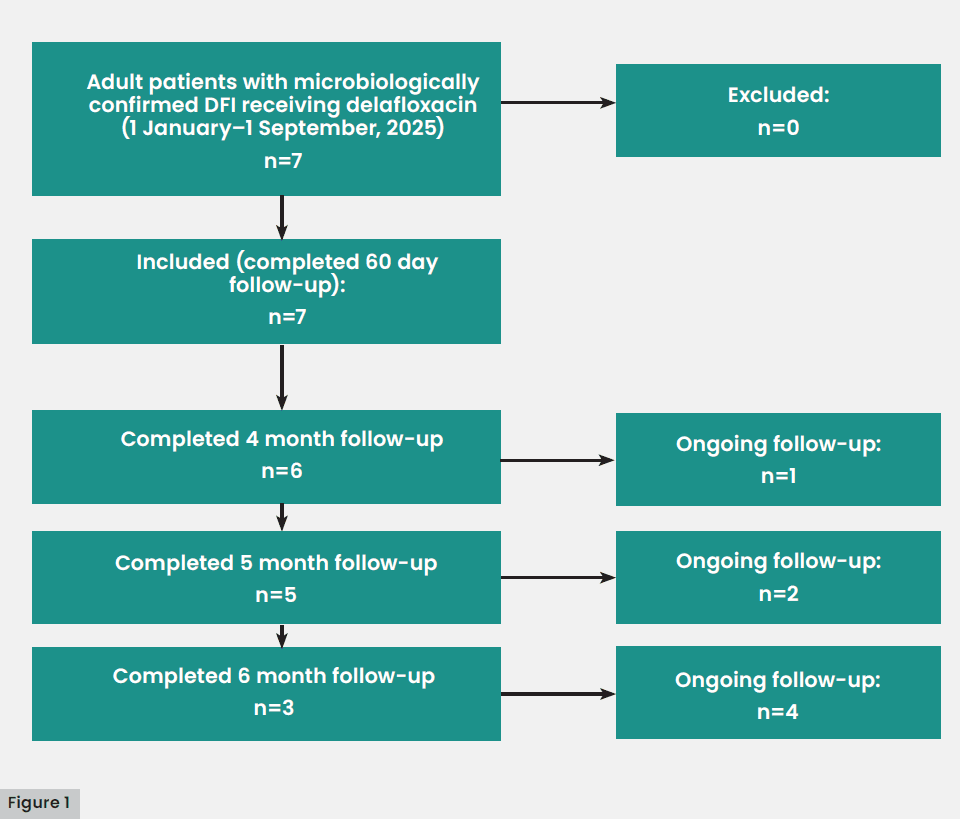
Figure 1. STROBE flow-chart of the study population
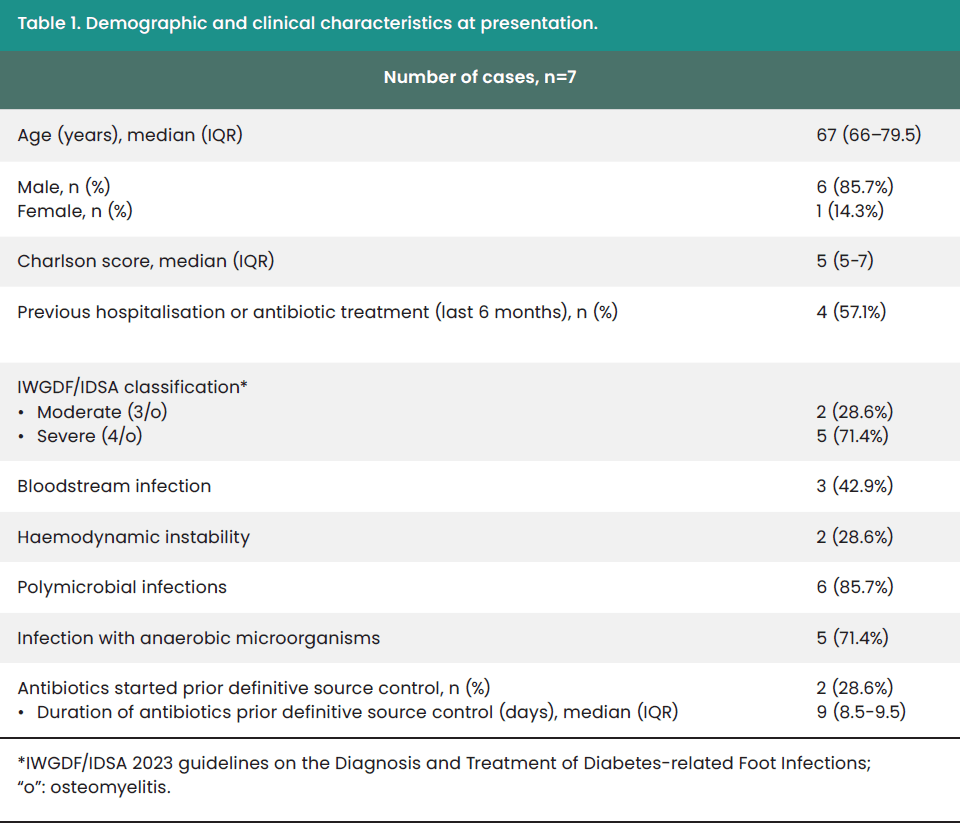
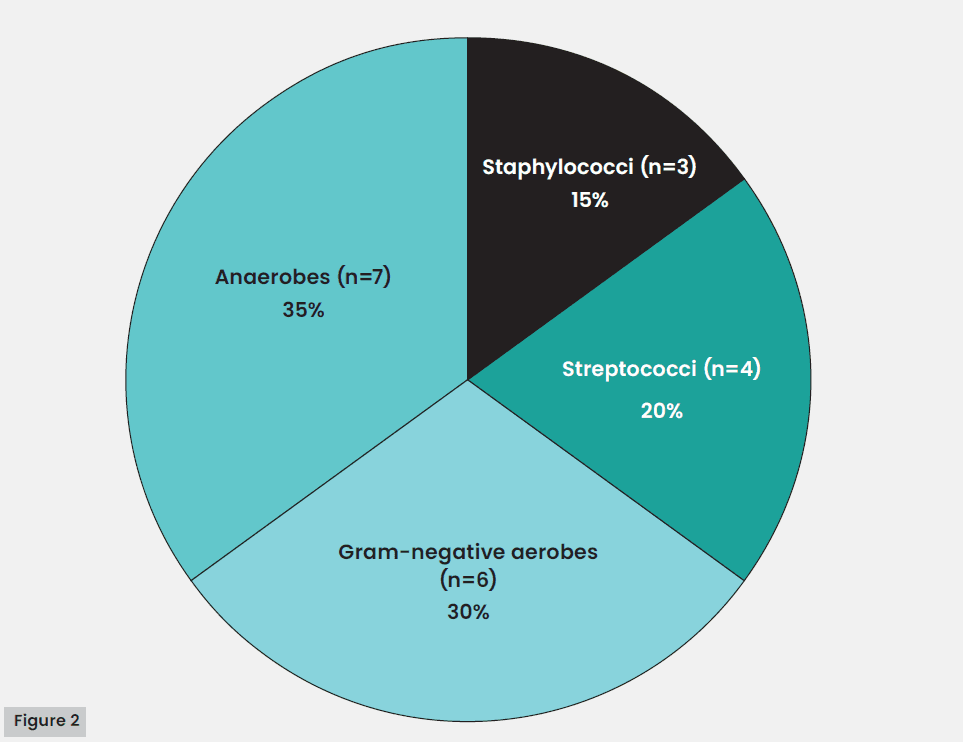
Figure 2. Summary of microbiological isolates (n=20; Specific isolates: MSSA=1, MRSA=2, S. agalactiae=1, S. anginosus=1, S. canis=1, E. faecalis=1, E. coli FQ-R=1, E. coli FQ-S=1, Morganella morganii=2, K. pneumoniae FQ-R=1, Acinetobacter iwofii=1; Finegoldia magna=1; Peptoniphilus assacarolyticus=2, Prevotella bivia=2, Bacteroides fragilis=2). (MSSA: methicilin-susceptible S. aureus; MRSA: methicilin-resistant S. aureus; FQ-R: documented resistance to levofloxacin and/or ciprofloxacin).
All patients underwent surgical debridement and intraoperative microbiological sampling. Empirical therapy consisted mainly (4/7 cases, 57.1%) of piperacillin-tazobactam (loading dose 4.5 g, followed by maintenance dose of 18g in continuous infusion) plus daptomycin (8-10 mg/kg every 24 hours). Median time for the switch from IV to oral therapy and discharge was 12 days (7.5–12.5 days). At discharge, all patients switched to monotherapy with oral delafloxacin (450 mg every 12 hours), prescribed for a median of 21 days (IQR 18–22). The median overall duration of antibiotic treatment was 28 days (IQR 28–30.5) [Table 2]. No deviations from the treatment protocol (see “Multidisciplinary treatment protocol” section) were recorded.
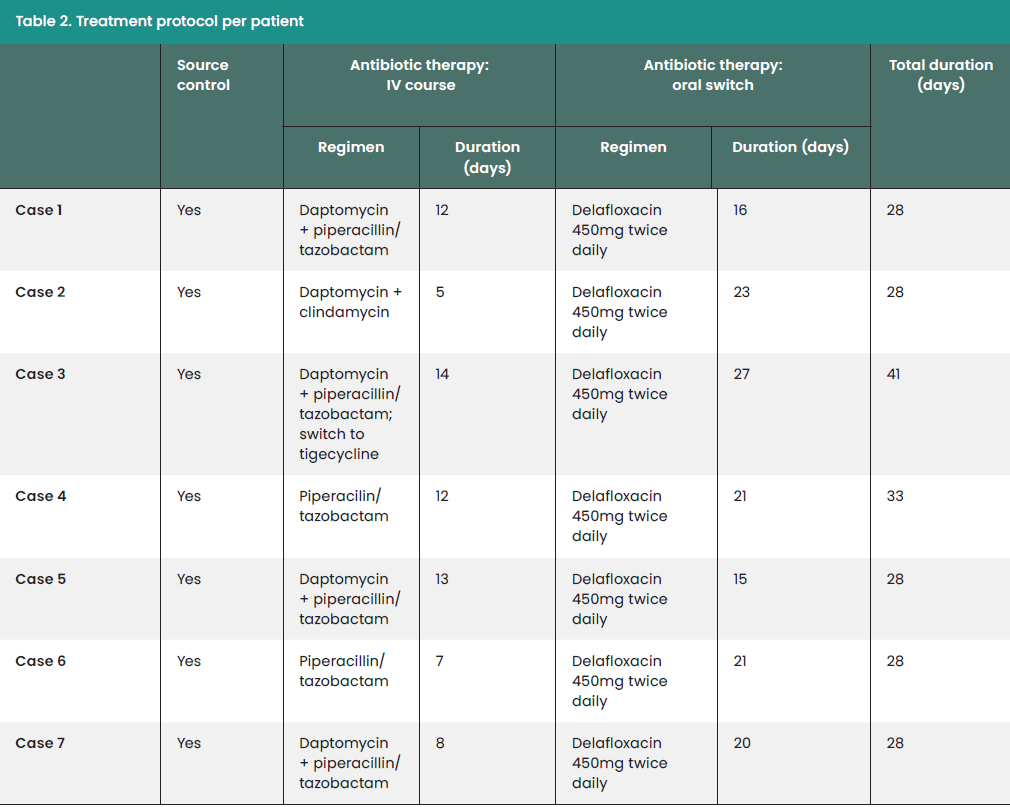
Table 2: Dosages: piperacillin/tazobactam loading dose 4.5 g followed by maintenance dose of 18 g in continuous infusion; daptomycin 8-10 mg/kg every 24h; clindamycin 600 mg every 6h; tigecycline first dose 100 mg and following doses 50 mg every 12h.
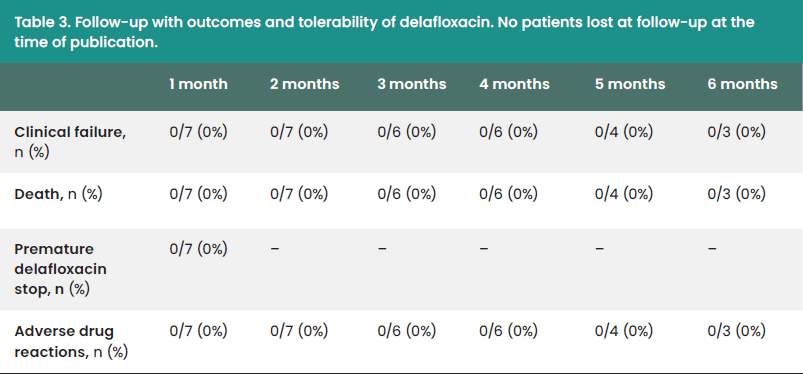
All patients completed the delafloxacin course and any adverse drug reaction (ADR) or tolerability complaint were reported. At 2 months follow-up, no cases (0/7) of failure have been observed. Among the three patients who completed 6 months follow-up, no treatment failures have been recorded. No patients were lost at follow-up [Table 3].
Literature review
To date, in the literature only a single case report of delafloxacin use in DFI is described (Serrudo et al, 2024). It refers to an 80-year-old male patient who underwent trans-metatarsal amputation and received delafloxacin 450 mg twice daily IV. P. aeruginosa, E. faecalis and E. coli were isolated from bone specimens. As the report focuses on advanced wound healing, the authors did not report either the duration of antibiotic treatment neither if any related ADR occurred.
Discussion
We presented the characteristics and outcomes of seven cases of moderate to severe DFI treated with oral delafloxacin. Evidence regarding delafloxacin use in osteoarticular infections is still scarce (Hornak and Reynoso, 2022; Vidwanset al, 2023; Serrudo et al, 2024) and, to our knowledge, no consistent reports specifically addressing DFIs have been published to date. Moreover, delafloxacin is not mentioned in two recent reviews on novel treatment options and oral antibiotic therapies in DFIs (Gachet et al, 2025; Jing et al, 2025).
Hornak and Reynoso (2022) described two cases of prosthetic joint infections (PJIs), both caused by methicillin-resistant S. epidermidis, treated with delafloxacin. Vidwans et al (2023) reported a single case of P. aeruginosa osteomyelitis where delafloxacin was used. Treatment duration ranged from 28 to 115 days, with favourable outcomes and no adverse events. In a paper evaluating the in vitro activity of delafloxacin against S. epidermidis strains isolated from osteoarticular infections, two cases of S. epidermidis PJIs cured with delafloxacin plus rifampin were also mentioned (Tessier et al, 2024). However, clinical details and antibiotic duration, were not provided.
DFIs are characterised by the concomitant presence of several pathogenetic factors, such as peripheral neuropathy, local ischaemia, frequent healthcare interactions, and presence of chronic diabetic foot ulcers (DFUs) associated with biofilm production and complex bacterial communities development (Macdonald et al, 2021). Our findings are in line with those already reported in the literature regarding the frequent presence of polymicrobial communities (86% in our case-series) with high prevalence of anaerobes (71.4% in our series) in DFIs (Macdonald et al, 2021; Villa et al, 2024). The role of anaerobes is increasingly recognised as non-culture-based diagnostic methods (i.e. 16S rRNA gene sequencing) which can improve the limited sensitivity of conventional anaerobic cultures. A recent meta-analysis confirmed the better ability of molecular methods, compared to culture-based ones, to identify anaerobic microorganisms from DFI and diabetic foot ulcers samples (83.8% [52.5-100%] versus 7.45% [0-53.3%]) (Villa et al, 2024).
Delafloxacin exhibits excellent activity against Gram-positive bacteria (S. aureus, coagulase-negative Staphylococci, S. pneumoniae, among others), Gram-negative pathogens (Enterobacterales and P. aeruginosa, among others) and is very active against both Gram-positive and Gram-negative anaerobes, such as C. difficile, P. acnes, C. perfringens, B. fragilis, Prevotella spp and Fusobacterium spp. (Sillerströmet al, 2004; Gómez-Zorrilla et al, 2022; Cobo et al, 2024). Its broad-spectrum coverage and the anti-anaerobic activity, make delafloxacin a promising option for DFI management.
In our cohort, over half of the patients had a recent hospitalisation or antibiotic exposure, both recognised risk factors for antimicrobial-resistance (Li et al, 2025). A concerning rise in resistance patterns, including resistance to traditional FQs, have been described among DFI isolates (Soldevila-Boixader et al, 2025; Zambelli et al, 2025). In this context, it should be highlighted that delafloxacin efficacy has been demonstrated in FQ-resistant strains, even in S. aureus isolates harboring the mecA gene (Ribeiro et al, 2024). Thus, delafloxacin might represent a suitable option in case of strains resistant to other FQs. In vitro studies analysing Staphylococcus strains resistant to other FQs (ofloxacin or levofloxacin) isolated from osteoarticular samples, have shown wide variation in delafloxacin susceptibility (48.2–89.1%, adopting a MIC threshold of 0.25; 1–3.9%, adopting a MIC threshold of 0.016; Loïez et al, 2024; Tessier et al, 2024). It should be noted that interpretation of delafloxacin susceptibility for coagulase negative Staphylococci (CoNS) is challenging, as no official breakpoints are available from EUCAST. In previous studies, S. aureus breakpoints have been arbitrarily applied to CoNS isolates (Loïez et al, 2024; Tessier et al, 2024).
In our case series, ciprofloxacin-resistant Enterobacteriaceae (E. coli and Klebsiella pneumoniae) were isolated from two patients. Both achieved a favourable outcome after delafloxacin treatment. Unfortunately, delafloxacin susceptibility could not be assessed as the E-test was unavailable in our laboratory at the time of isolation.
DFIs often represent acute exacerbations of chronic DFUs or osteomyelitis. These conditions are characterised by biofilm formation, where sessile bacteria, small-colony variants and intracellular forms contribute to persistence and antimicrobial tolerance (Senneville et al, 2023). Antibiotics with anti-biofilm activity and intracellular activity, such as FQs, may therefore play a role in this disease (Zelmer et al, 2022). Delafloxacin has shown promising in vitro anti-biofilm activity against P. aeruginosa, and strong intracellular penetration, particularly in S. aureus infections (Craddock et al, 2023; Tudahl et al, 2025).
FQ are known to exhibit a great tissue diffusion also in difficult-to-reach sites, such as bone and joints (Metallidis et al, 2007; Thabit et al, 2019). Although clinical data and bone penetration of delafloxacin in humans are lacking, preliminary murine models suggest a good bone penetration (Mogle et al, 2018). Some evidence exists that, at least in S. aureus strains, exposure to sub-MIC concentrations of delafloxacin increases the biofilm formation (Bodo et al, 2019). In order to prevent resistance emergence and clinical failure, reliable PKPD parameters development might be very useful for a safe use of delafloxacin in osteoarticular infections. To our knowledge however, no PKPD models are available at the moment.
Compelling evidence have shown that early switch to oral therapy in osteomyelitis, even in diabetic patients, is as effective as IV-only therapy (Gachet et al, 2025; Kipp et al, 2025). Oral therapy is associated with fewer costs and adverse events related to hospitalisation and catheter-related complications. Thus, drugs with excellent oral bioavailability, such as FQs, tetracyclines, oxazolidinones and rifampin, represent a good option for early patient discharge. Delafloxacin oral bioavailability is hovering around 59%, which explains the different IV (300 mg every 12 hours) and oral dosages (450 mg every 12 hours). In our case series, oral switch was always associated with hospital discharge, likely improving patient’s satisfaction and safety.
No ADRs or tolerability problems have been reported in our case-series, even in patients exceeding the recommended duration of 14 days. None of them exhibited gastrointestinal disorders (diarrhoea, nausea and vomiting), that are the most common ADRs reported in clinical trials.
As QT prolongation (>440 ms) occurs in up to 44% of patients with type 2 diabetes (T2D), concerns about FQs use (associated with QT prolongation) in this population may arise (Ninkovic et al, 2016). Thus, it is reassuring that delafloxacin has not been associated with QT interval prolongation from phase I, II and III trials (Gómez-Zorrilla et al, 2022).
Others FQs have been associated with dysglycaemia in people with diabetes (Heurtebize and Faillie, 2024). So far, hypoglycaemia or hyperglycaemia attributable to delafloxacin has rarely been reported (Gómez-Zorrilla et al, 2022; Guo et al, 2024). Considering that up to 89% of T2D patients receive ≥ 5 medications at some point and polypharmacy is increasing, antibiotics with few drug-interactions are preferable in this population (Johansson et al, 2024). Of note, no drug interactions alerts exist for delafloxacin and antidiabetic drugs.
Our case series has several limitations, including the small sample size, lack of a control group due to the study design, and incomplete 6 months follow-up, all of which limits the generalisability and precludes definitive conclusions. In all cases delafloxacin was used empirically, as EUCAST published delafloxacin breakpoints only for a minority of microorganisms (S. aureus in the context of ABSSSI and CAP, Streptococcus A, B, C and G, S. anginosus and E. coli) and susceptibility testing became available in our laboratory from August 2025.
The strengths of the study include the adoption of strict inclusion criteria (proven microbiological diagnosis of DFI with osteomyelitis) that excluded superficial infection, colonisations or equivocal diagnosis, the application of a standardised treatment protocol combining surgery and antibiotic therapy, and a rigorous prospectively implemented follow-up strategy.
Conclusion
Delafloxacin’s broad spectrum of activity—including excellent efficacy against anaerobes, together with the availability of an oral formulation, presumptive good bone penetration, minimal drug–drug interactions, and high tolerability, represent key advantages supporting its potential role in the treatment of DFIs. Despite the limitations of our study, namely the small sample size and absence of a control group, our findings provide preliminary real-world evidence supporting delafloxacin as a safe and effective oral step-down option for moderate to severe DFIs with bone involvement.
