Development and overview of international recommendations for therapeutic wound and skin cleansing
Received:
Accepted:
Published:
Authors: Emily Haesler, Terry Swanson, Dot Weir, Geoff Sussman, Donna Larsen
Citation:
Haesler E et al, (2026) Development and overview of international recommendations for therapeutic wound and skin cleansing. Global Wound Care Journal 2 (1): 40-47.
Funding:
The IWII received funding support from B.Braun, Convatec, Hartmann, Mölnlycke and Urgo Medical to develop Therapeutic wound and skin cleansing: Clinical evidence and recommendations. The views expressed in document are those of the IWII Expert Working Group. No funding was received for preparation of this article.
Acknowledgements:
The IWII Expert Working Group consisted of Emily Haesler (Australia), Terry Swanson (Australia) Karen Ousey (UK), Donna Larsen (Australia), Geoff Sussman (Australia), Dot Weir (USA), Keryln Carville (Australia), Patricia Idensohn (UK), Susie Seaman (USA), Paulo Alves (Portugal), David H. Keast (Canada), Kimberly LeBlanc (Canada), Harikrishna Nair (Malaysia), Steven Percival (UK) and Nicola Waters (Canada). Lindsay Kalan (Canada) and Thomas Bjarnsholt (Denmark) reviewed the document, provided comment and assisted with science-based inquires.
Participants in the Delphi process were The IWII Expert Working Group listed above, with Leanne Atkin (UK), Nicoletta Frescos (Australia) and Nanthakumahrie Gunasegaran (Singapore).
The IWII Expert Working Group acknowledge and thank the following group members who provided wound photography to enhance the document: Donna Larsen (Australia), Dot Weir (USA), Patricia Idensohn (South Africa), Terry Swanson (Australia) and Kimberly LeBlanc (Canada).
Corresponding author:
Emily Haesler emily.haesler@curtin.edu.au
DOI:
10.63896/gwcj.2.1.40
Therapeutic wound cleansing is a crucial and fundamental component of effective wound care yet remains inconsistently understood and performed across clinical settings and international contexts. In response to this inconsistency, the International Wound Infection Institute (IWII) convened a multidisciplinary Expert Working Group to review the best available evidence and develop practical, evidence-based recommendations. This review outlines the development of Therapeutic wound and skin cleansing: Clinical evidence and recommendations, a resource that integrates research findings, expert consensus, and clinical tools. The project involved a systematic literature review and a Delphi consensus process to define key terminology and establish 13 practice recommendations. These recommendations address optimal cleansing frequency, aseptic technique selection, choice and safety of cleansing solutions, and strategies for pain management. A novel three-zone model for therapeutic cleansing is presented, alongside consensus definitions for terms such as periwound, toe flossing and limb hygiene. The document highlights gaps in current knowledge, particularly regarding wound bed pH and the therapeutic index of antiseptics and identifies areas for future research. By providing comprehensive guidance and practical resources, the IWII aims to standardise therapeutic wound cleansing practices globally and improve patient outcomes.
The fundamental components of wound care – cleansing and protecting the wound bed – have been known since the earliest human civilizations, with documented evidence of these practices dating to 2100BC (Broughton et al, 2006). Therapeutic wound cleansing, defined as the active removal of surface contaminants, loose debris, non-attached non-viable tissue, microorganisms and/or remnants of previous dressings from the wound bed and periwound, is a fundamental component of the wound dressing procedure – a process that is performed to prepare and support the wound bed for healing (Rodeheaver et al, 2018; International Wound Infection Institute [IWII], 2025).
The wound dressing procedure incorporating wound cleansing continues to be foundation knowledge within nursing and other health professions. However, the way in which we perform this important procedure has evolved alongside our knowledge and understanding of germ theory, asepsis, moist wound healing, the wound infection continuum and wound hygiene. Despite these significant paradigm shifts, it is not uncommon for a wound dressing procedure to be taught and performed as a ritualistic task, rather than as a skilled process that requires a strong understanding of the underpinning theoretical frameworks, application of clinical judgement and competency in complex procedures in order to achieve therapeutic outcomes (Blunt, 2001; Barber, 2002). Additionally, the wound cleansing solutions used in the process have progressed from beer, hot water, wine, vinegar and oil used by ancient civilisations, to potable water and plant-based salves (still used in low-resource regions), early antiseptics and a now myriad of contemporary antiseptic solutions that are available (Forrest, 1982; IWII, 2022).
In contrast to its often ritualistic or inadequate performance, correctly performed wound cleansing uses an appropriate technique and solution that is therapeutic for the tissue within and around the wound and promotes the healing process. Referred to as therapeutic wound cleansing, the procedure should achieve removal of undesirable surface contaminants (e.g. wound exudate), loose debris, non-attached and non-viable tissue, microorganisms, and remnants of previous wound dressings from the wound bed and the periwound using a wound cleansing solution and mechanical action (consensus definition; Nair et al, 2023, Ringblom et al, 2024). By removing non-viable tissue and debris, the wound bed is rendered less conducive to proliferation of microorganisms and to the pro-inflammatory response, thereby promoting the healing process (Wilkins et al, 2013; Weir et al, 2019; Torkington-Stokes et al, 2024).
In addition, therapeutic wound cleansing may reduce wound-related pain, exudate and odour, increase the individual’s comfort and cleanliness and promote wound assessment by improving visualisation of the wound bed and wound edges (Wilkins et al, 2013; Collier et al, 2017, Weir et al, 2019). To achieve these outcomes, consideration is required to selecting an appropriate cleansing solution, appropriate medical equipment to perform the procedure and application of an appropriate technique, with selection of all three based on the individual, their wound and the context (McLain et al, 2021). Therapeutic wound cleansing is closely aligned with, but different from, general skin hygiene and washing the surrounding skin.
In 2023, an international, multidisciplinary panel of experts from the IWII identified that there was significant variation across geographic and clinical settings in the way in which wound cleansing is performed. Although our understanding of the importance of wound cleansing as a critical component of wound bed preparation is universally acknowledged, there was a need to analyse the best available evidence addressing questions associated with wound cleansing, and for practical guidance on best practice in how it is performed. To address this perceived need, an IWII Expert Working Group undertook to develop a back-to-basics resource for use in clinical practice and as an education resource about the latest and most effective wound cleansing techniques. This paper discusses the development of this resource, Therapeutic wound and skin cleansing: Clinical evidence and recommendations (IWII, 2025).
Aim
The aim of the project was to establish evidence-based recommendations for wound cleansing to promote consistency in clinical practice across clinicians, clinical settings and patient contexts, thereby improving outcomes for individuals with a wound. The project objectives included:
- Review the highest-level evidence on wound cleansing to inform the development of evidence-based recommendations for clinical practice.
- Reach consensus agreement on terminology associated with wound cleansing.
- Stimulate further research and innovation in wound cleansing by highlighting areas for improvement and/or in which limited evidence is available.
Methods
Developing inquiry questions
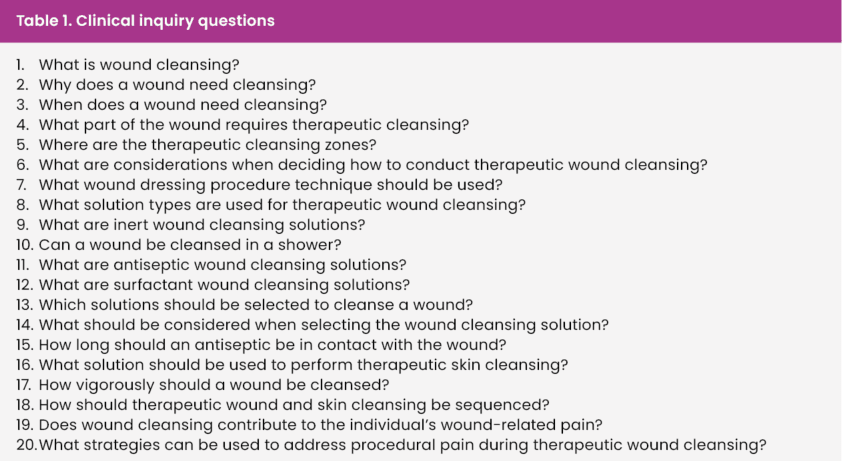
In the first stage of the document development, the IWII Expert Working Group participated in a roundtable discussion to identify issues related to wound cleansing for which there is inconsistent understanding and/or practice that could be improved with evidence-based recommendations. The Expert Working Group also developed a list of terms for which consensus definitions were required, planned resources to accompany the practice recommendations and developed inquiry questions [Table 1] to use as a framework for reviewing the literature and developing recommendations.
Literature identification and appraisal
A systematic search was conducted in Medline, PubMed, Embase, Cochrane Library and Google Scholar to identify research relevant to each inquiry question. The search strategy used MeSH terms and EBSCO terms that were adapted for other databases. The controlled vocabulary searches covered the following:
- Wound cleansing, cleaning, cleanse, wound irrigation, asepsis, cleansing, shower, technique, therapeutic cleansing, cleansing solution.
- Wound, wound care, chronic wound, surgical wound.
- Antimicrobials, antimicrobial, topical agent, antiseptic, surfactant.
Targeted searches of wound-focused websites were undertaken to identify relevant consensus documents and statements. Seminal papers were added to those identified in the literature search. The search was limited to reports in English since 2000 that addressed human subjects or bench science.
Identified evidence was screened for relevance to the inquiry questions. All identified sources were classified using the Joanna Briggs Institute (2013) Levels of Evidence for Effectiveness [Figure 1], and this ranking was used to identify the type of studies underpinning each recommendation. Where higher level evidence was identified as addressing the clinical question, evidence at lower level on the hierarchy was excluded, excepting where it contributed unique discussion points.
Delphi process
The 15-member IWII Expert Working Group undertook a consensus process with a goal of attaining agreement on standardised definitions for terminology associated with wound cleansing. The consensus process extends work the IWII has been undertaking since 2016 to build a consensus-based wound infection-related glossary (IWII, 2016; Haesler et al, 2022).
The IWII Expert Working Group used an online application of the RAND/UCLA Appropriateness Method, a Delphi method for reaching formal agreement on the interpretation of science, for which validity and reliability has been reported (Fitch et al, 2001; IWII, 2016; Haesler et al, 2019). The IWII has previously reported in detail how the online application is implemented, and how agreement is determined using the RAND/UCLA Appropriateness Method (IWII, 2016; Haesler et al, 2019; 2022).
For this project, the IWII used the same process to establish consensus definitions for the following six wound cleansing terms: periwound, debridement, limb hygiene, toe flossing, therapeutic wound cleansing and mechanical cleansing. In addition to the IWII Expert Working Group, three external researchers with expertise in therapeutic wound cleansing participated in the Delphi process, increasing representation from different clinical disciplines and geographic regions (see the acknowledgements).
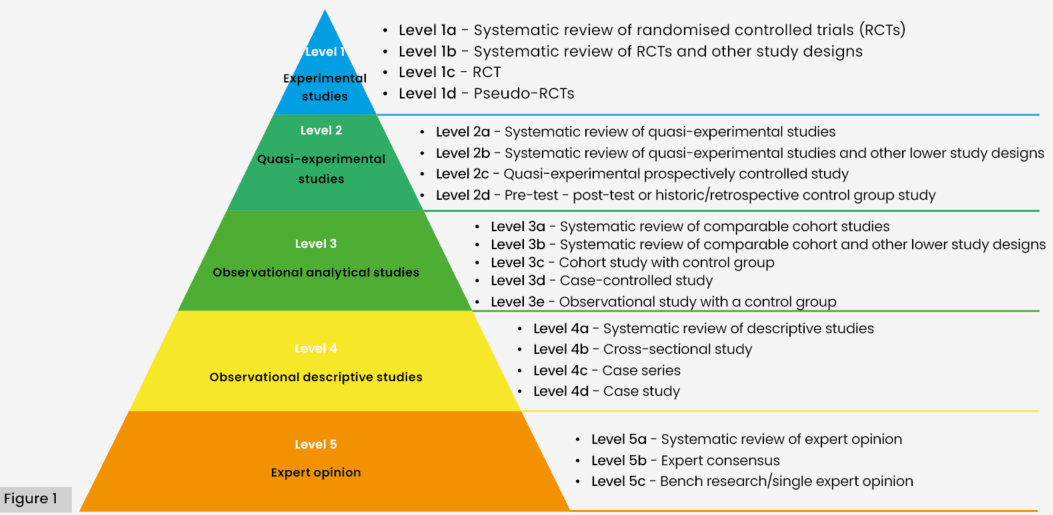
Figure 1: Joanna Briggs Institute: Levels of Evidence for Effectiveness. Adapted from: Munn Z, Lockwood C, Moola S (2015) The Development and Use of Evidence Summaries for Point of Care Information Systems: A Streamlined Rapid Review Approach. Worldviews Evid Based Nurs 12(3): 131-8
Results
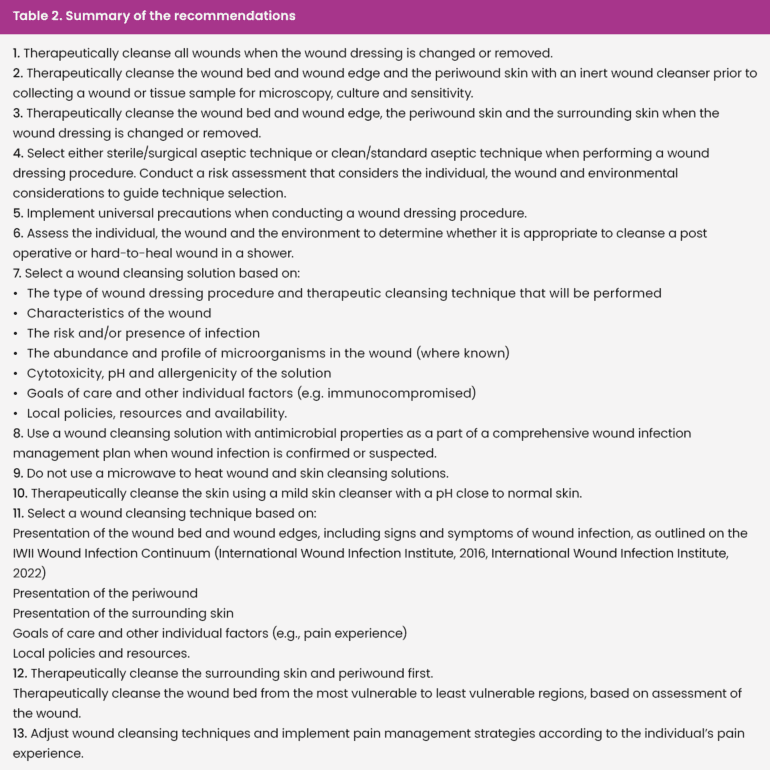
Consensus definitions were agreed upon for five wound cleansing terms: periwound, debridement, limb hygiene, toe flossing and therapeutic wound cleansing. These definitions have been identified in the introduction and throughout these results and are available in Therapeutic wound and skin cleansing: Clinical evidence and recommendations. Thirteen recommendations focused on therapeutic wound cleansing were made [Table 2].
Timing of wound cleansing
Several recommendations addressed the timing of therapeutic wound cleansing. Only one cohort study was identified that explored whether cleansing a wound was more effective than leaving the wound bed untouched (Yoshikawa et al, 2024). The results suggested that therapeutic wound cleansing was associated with faster healing (Level 3 evidence).
Another small cohort study found that microbial counts at the periwound skin and surrounding skin are immediately reduced by wound cleansing that includes these regions (Konya et al, 2005). However, microbial levels took only 24 hours to return to pre-cleansing levels (Level 3 evidence).
Based on this evidence, the IWII Expert Working Group recommends that therapeutic wound cleansing is performed every time a wound dressing is removed and/or changed.
Therapeutic wound cleansing zones
The IWII Expert Working Group recommends that therapeutic wound cleansing should include three therapeutic cleansing zones: the wound bed and edge, the periwound skin and the surrounding skin. These three wound zones or regions are defined as the wound bed and its demarcating wound edge (zone 1), the periwound skin (zone 2), which the IWII xpert Working Group reached agreement as being from the wound edge to 4 cm beyond the wound edge (consensus definition), and the surrounding skin (zone 3, extending to 20 cm beyond the wound edge). Noting that the international literature includes a range of definitions for these regions, the Delphi process was undertaken to reach agreement on the meaning of periwound skin, concluding the defined 4 cm region (LeBlanc et al, 2021). Within Therapeutic wound and skin cleansing: Clinical evidence and recommendations (IWII, 2025) these regions are illustrated [Figure 2].
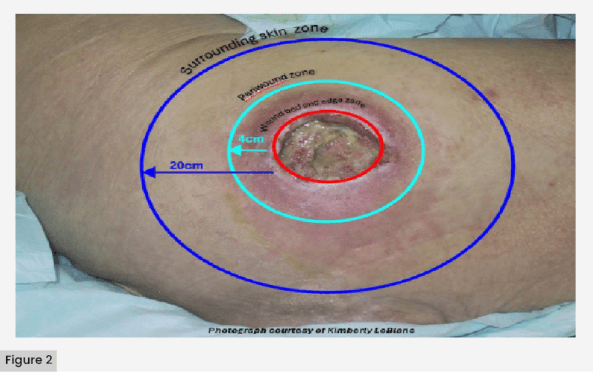
Figure 2. Therapeutic cleansing zones.
Wound cleansing technique
Several recommendations addressed the techniques important to perform the wound dressing procedure. Selection of the most appropriate aseptic technique has been a long-term debate in wound care.
A systematic review and meta-analysis suggested that a sterile/surgical aseptic technique and a clean/standard aseptic technique are not substantially different in their effectiveness in preventing wound infection (Level 1 evidence; Purssell et al, 2024).
Another systematic review outlined the scientific basis of infection control, including recognised strategies to reduce cross-contamination and healthcare-associated infections (Level 1 evidence; Lommi et al, 2023).
Based on this evidence, the IWII Expert Working Group recommends aseptic technique be selected based on a risk assessment that considers the individual, their wound and the environment, and that universal precautions should always be implemented.
Wound cleansing solutions
Several recommendations addressed selection of a wound cleansing solution in wounds with confirmed or suspected wound infection, or at risk of infection.
A systematic review and meta-analysis showed no substantial difference in wound infection rates when using a sterile solution versus potable water, although the context is important to these findings (e.g. likely low baseline risk of infection in study participants) (Level 1 evidence; Fernandez et al, 2022).
Several meta-analyses showed no substantial difference in post-operative infection rates between wounds cleansed in a shower in the early days post-operatively and delaying showering for over 7 days (Copeland-Halperin et al, 2020; Ren et al, 2024).
Several systematic reviews reporting outcomes using antiseptics for wound cleansing showed these products are generally effective in reducing microbial burden and reducing clinical signs and symptoms of wound infection in wounds with confirmed or suspected infection or at risk of infection (Level 1 evidence; Norman et al, 2016; McLain et al, 2021; Soeselo et al, 2022; Ringblom et al, 2024). Additional evidence indicated that topical antiseptics also play a role in suppressing the development of biofilm in wounds with confirmed or suspected infection or at risk of infection (Beam, 2008; Cornish et al, 2016).
Based on this evidence, the IWII Expert Working Group recommends that wound cleansing with water in a shower could be used for select individuals determined through a comprehensive individualised assessment of the wound and clinical context (examples include, but are not limited to, community versus inpatient setting, post-operative versus chronic wound; IWII, 2022). This could be facilitated by the use of a suggested assessment tool (IWII, 2022). Other wound cleansing solutions (e.g. sterile inert solutions or antiseptic wound cleansers) should be selected based on the appropriate aseptic technique, the wound presentation, characteristics of the solution, goals of care and contextual factors (examples include, but are not limited to, the clinical care setting, accessibility to different wound cleansing solutions and facility-based policies). However, when wound infection is confirmed or suspected, a wound cleansing solution with antiseptic properties should the first line choice to cleanse the wound bed, the wound edge and the periwound region.
Regardless of the cleansing solution, the IWII Expert Working Group recommend that a microwave not be used to warm the fluid due to the risk of overheating the fluid and causing a burn injury (Expert opinion).
Cleansing the surrounding skin
The importance of cleansing the surrounding skin to remove wound dressing debris, hyperkeratotic tissue, and accumulated dirt and sebum was supported by the literature. The IWII Expert Working Group reached consensus that the term limb hygiene refers to the cleansing and drying of a limb to achieve and maintain skin integrity (consensus definition), and that this process may include toe flossing, which was defined as the action of cleansing and drying between the toes, usually with moistened gauze, cloth or a device designed for the purpose (consensus definition). A systematic review (Level 1 evidence) supported a recommendation to use a skin cleanser with a pH close to that of normal skin when performing limb hygiene/cleansing the surrounding skin (Lichterfeld et al, 2015).
Managing wound pain during cleansing
A systematic review synthesising studies on managing wound-related procedural pain indicated that a range of non-pharmacological and pharmacological strategies are appropriate and effective for managing pain that can arise from the wound dressing procedure (Level 1 evidence; Admassie et al, 2022). This evidence supported a recommendation to adjust the wound cleansing technique and to implement individualised interventions to prevent and treat pain.
Discussion
The aim of the project was to reach agreement on definitions for terms associated with wound cleansing and to establish evidence-based recommendations for wound cleansing. The recommendations highlight the wide range of wound cleansers available, with differing characteristics that need to be evaluated in context and individualised. This includes considering the need for surfactant and antiseptic properties. To assist clinicians in evaluating the applicability of specific wound cleansers for the needs of an individual, the IWII Expert Working Group has compiled profiles of commonly used wound cleansing solutions, including their modes of action, concentrations and broad safety profiles. The therapeutic index has been proposed as one indicator that can be used to evaluate the relative safety of antiseptics (Geng et al, 2024). A therapeutic index is a quantitative value indicating the ratio of the therapeutic effect and toxic effect, with a value greater than 1 indicating that the antiseptic has broad-spectrum activity against microorganisms and a low level of cytotoxicity to mammalian cells (Geng et al, 2024, Kramer et al, 2018, Eriksson et al, 2022). However, a substantial proportion of the evidence providing an understanding of the minimal bactericidal concentration, as well as the safety profile (particularly cytotoxicity) of antiseptics is laboratory and/or animal-based (Schwarzer et al, 2020). The way microbes behave in human wounds varies from laboratory settings (Bjarnsholt et al, 2021), and the evidence should be applied with careful consideration to the clinical context. The therapeutic index is only one factor that might be considered when selecting a cleansing solution, and use of this index requires further research.
Another area requiring further research is the wound bed pH, including the differences observed between chronic and acute wounds, the change in wound bed pH throughout the healing process, and the effectiveness of applying antiseptics to optimise wound bed pH. The IWII Expert Working Group have proposed wound bed pH monitoring using pH strips, meters or sensors, as a possible consideration when selecting an antiseptic; however, the evidence is insufficient to make a recommendation on this topic. A greater understanding of the impact of a cleansing solution on the wound bed pH in the clinical context and the role this may play in healing would inform the development of future recommendations.
The IWII Expert Working Group was unable to reach consensus on a definition of mechanical cleansing. Though the Delphi process, the experts confirmed an understanding that therapeutic wound cleansing and debridement intersect on occasion. Debridement refers to removal of devitalised (non-viable) tissue from or adjacent to a wound, also removing foreign matter, exudate and microorganisms from the wound bed and promoting a stimulatory environment (consensus definition).
The Delphi participants had mixed opinions on whether the application of more significant mechanical force during therapeutic wound cleansing in order to dislodge debris and non-viable tissue should be defined as cleansing or debridement. The intersection between the three key activities making up the wound dressing procedure (therapeutic wound cleansing, debridement and wound dressing application) is illustrated in the IWII’s theoretical model of optimal wound care presented in Therapeutic wound and skin cleansing: Clinical evidence and recommendations (IWII, 2025).
The recommendations highlight that the evidence suggests that many therapeutic wound cleansing techniques and cleansing solutions will prepare the wound bed for healing and achieve positive patient outcomes. To assist clinicians in making informed clinical decisions, the IWII Expert Working Group has provided several resources. The document presents a new IWII Wound Cleansing Continuum that integrates clinical guidance on selecting wound cleansing techniques and cleansing solutions with the IWII’s Wound Infection Continuum, aligning wound cleansing practice with our scientific understanding of the presentation and progression of wound infection (IWII, 2025). Other resources include a decision tree and a table of common considerations when selecting a wound cleansing solution.
Conclusion
The IWII’s resource, Therapeutic wound and skin cleansing: Clinical evidence and recommendations, presents a comprehensive overview of the best available evidence underpinning the fundamental clinical skill of therapeutically cleansing a wound (IWII, 2025). Using a systematic process, 13 clinical recommendations for wound cleansing were developed, with resources to assist in their implementation. A Delphi process achieved consensus agreement on five terms associated with therapeutic wound cleansing. Further research on the optimal frequency of therapeutic wound cleansing and on the most effective sequencing for cleansing different regions of the wound bed, the peri-wound and the surrounding skin is required. The use of the therapeutic index and the wound bed pH to guide selection of wound care products also warrant further investigation.
